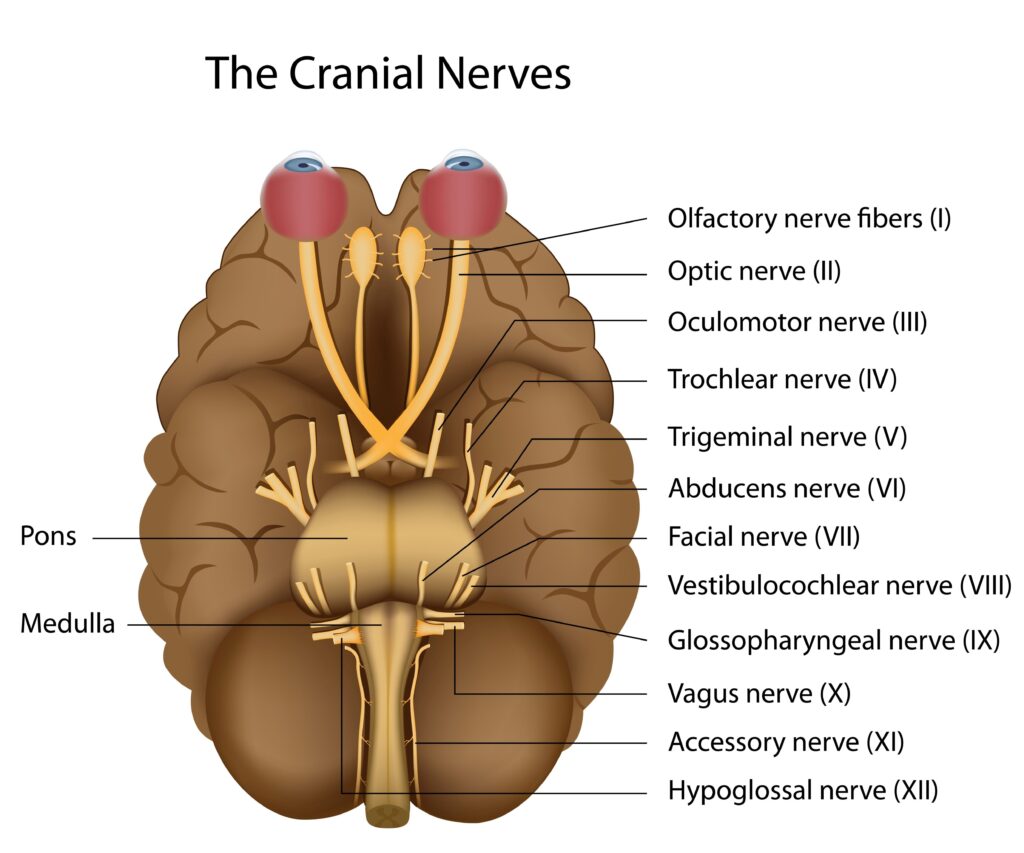
The Twelve Cranial Nerves: Functional Anatomy and Clinical Significance
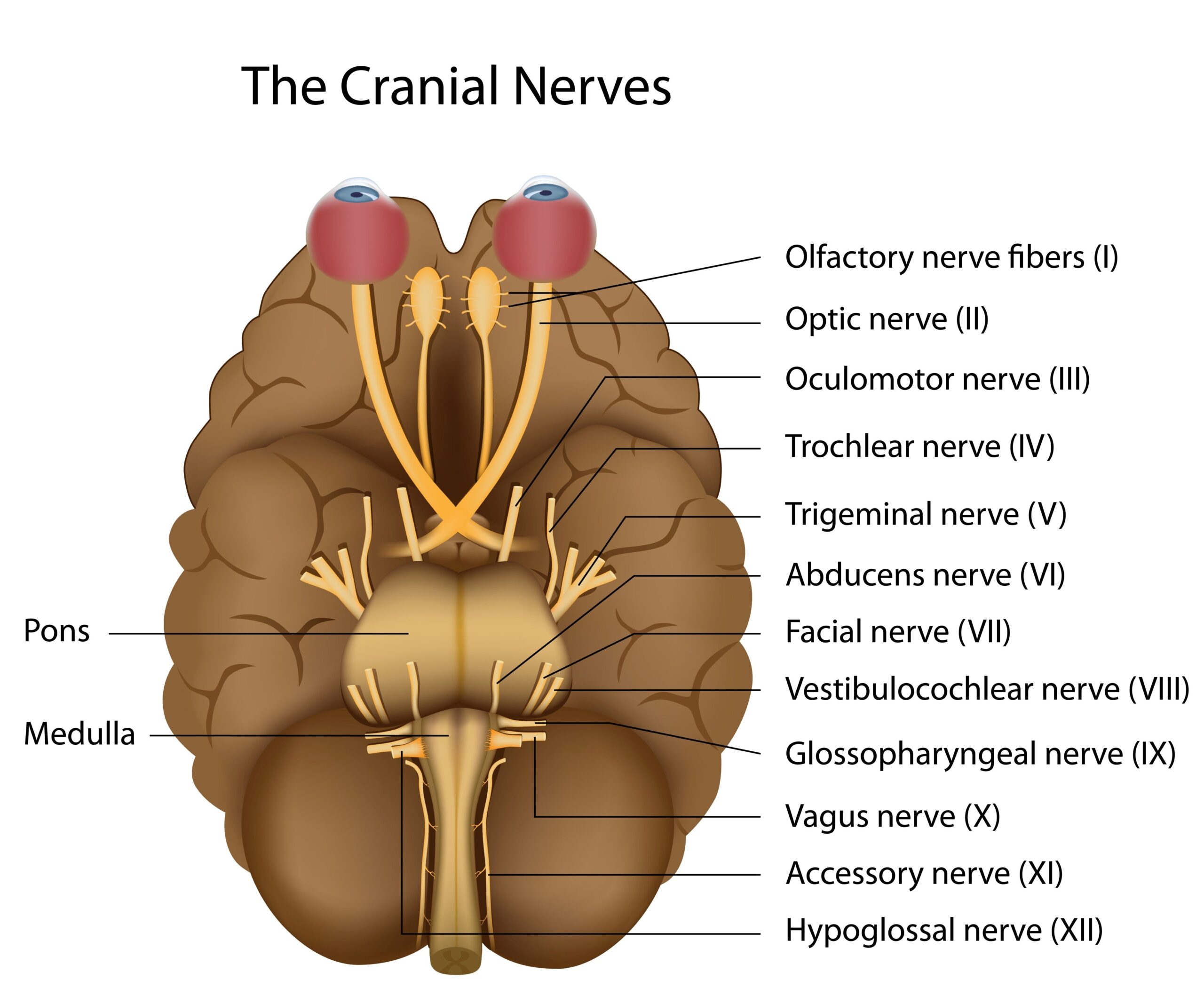
The cranial nerves are twelve pairs of nerves that emerge directly from the brain, primarily from the brainstem. These nerves are designated by Roman numerals I-XII, reflecting the order in which they exit the skull from anterior to posterior. Understanding cranial nerve anatomy and function is essential for clinical assessment and diagnosing various neurological conditions.
Olfactory Nerve (I)
The olfactory nerve is composed of special sensory fibers that mediate the sense of smell. These fibers originate from olfactory receptor cells in the nasal epithelium and project through the cribriform plate of the ethmoid bone to synapse in the olfactory bulb. Damage can result in anosmia (loss of smell), which may occur following head trauma, viral infections, or neurodegenerative disorders such as Parkinson’s disease and Alzheimer’s disease.
Optic Nerve (II)
The optic nerve carries special sensory fibers responsible for vision. Unlike typical nerves, the optic nerve is actually a tract of the central nervous system, containing axons from the retinal ganglion cells. These fibers project through the optic canal to the optic chiasm, where partial decussation occurs, and continue via the optic tracts to the lateral geniculate nucleus and ultimately the visual cortex. Damage can cause various visual deficits, including scotomas, hemianopsia, or complete blindness.
Oculomotor Nerve (III)
The oculomotor nerve contains somatic motor fibers that innervate four of the six extraocular muscles (superior, medial, and inferior recti, and inferior oblique) and the levator palpebrae superioris. It also carries parasympathetic fibers that control pupillary constriction and lens accommodation. Damage typically manifests as ptosis, diplopia, a “down and out” position of the affected eye, and pupillary dilation (mydriasis).
Trochlear Nerve (IV)
The trochlear nerve is the smallest cranial nerve and the only one to emerge from the dorsal aspect of the brainstem. It carries somatic motor fibers to the superior oblique muscle, which assists in downward and inward eye movement. Injury results in difficulty looking downward when the eye is adducted, causing vertical diplopia that worsens when looking down and to the contralateral side.
Trigeminal Nerve (V)
The trigeminal nerve is the largest cranial nerve and contains both sensory and motor fibers. It has three major divisions: ophthalmic (V1), maxillary (V2), and mandibular (V3). The ophthalmic and maxillary divisions are purely sensory, while the mandibular division contains both sensory and motor fibers. Sensory functions include facial sensation, corneal reflex, and proprioception from the jaw. Motor functions involve the muscles of mastication. Damage can lead to facial numbness, loss of corneal reflex, or weakness in jaw movement.
Abducens Nerve (VI)
The abducens nerve carries somatic motor fibers to the lateral rectus muscle, which abducts the eye. Damage causes medial deviation of the affected eye (esotropia) and horizontal diplopia that worsens when looking toward the affected side.
Facial Nerve (VII)
The facial nerve has complex functions, including motor innervation to the muscles of facial expression, parasympathetic fibers to the lacrimal, submandibular, and sublingual glands, and special sensory fibers for taste from the anterior two-thirds of the tongue. It also provides sensory innervation to parts of the external ear. Damage can result in facial weakness or paralysis (Bell’s palsy), reduced tear and saliva production, and altered taste perception.
Vestibulocochlear Nerve (VIII)
The vestibulocochlear nerve consists of two components: the vestibular nerve (balance) and the cochlear nerve (hearing). The vestibular component transmits information about head position and movement from the semicircular canals, utricle, and saccule. The cochlear component carries auditory information from the organ of Corti. Damage can cause vertigo, nystagmus, tinnitus, or hearing loss.
Glossopharyngeal Nerve (IX)
The glossopharyngeal nerve has mixed functions, including motor fibers to the stylopharyngeus muscle, parasympathetic fibers to the parotid gland, sensory fibers from the posterior third of the tongue, tonsils, and pharynx, and special sensory fibers for taste from the posterior third of the tongue. Damage can affect swallowing, taste perception, and the gag reflex.
Vagus Nerve (X)
The vagus nerve has the most extensive distribution in the body, providing parasympathetic innervation to thoracic and abdominal viscera, motor fibers to the pharyngeal and laryngeal muscles, and sensory and taste fibers from the pharynx, larynx, and epiglottis. It plays critical roles in speech, swallowing, and visceral functions. Damage can cause hoarseness, dysphagia, and various autonomic disturbances.
Accessory Nerve (XI)
The accessory nerve has cranial and spinal roots. The cranial component joins the vagus nerve and contributes to pharyngeal and laryngeal function. The spinal component innervates the sternocleidomastoid and trapezius muscles, controlling head rotation and shoulder elevation. Damage results in weakness of these muscles, affecting head turning and shoulder shrugging.
Hypoglossal Nerve (XII)
The hypoglossal nerve carries somatic motor fibers to the intrinsic and extrinsic muscles of the tongue, controlling its movement and shape. Damage causes tongue weakness and atrophy, with deviation toward the affected side upon protrusion due to unopposed action of the intact contralateral genioglossus muscle.
Clinical Assessment
Cranial nerve assessment is a fundamental component of the neurological examination. Systematic evaluation includes testing smell, visual acuity, visual fields, pupillary reflexes, extraocular movements, facial sensation, facial expression, hearing, balance, pharyngeal and palatal function, shoulder strength, and tongue movements. Localized or multiple cranial nerve palsies can provide valuable localizing information for neurological diagnosis.
Conclusion
The cranial nerves form an intricate network that mediates critical sensory, motor, and autonomic functions. Understanding their anatomy, function, and clinical implications is essential for accurate neurological evaluation and diagnosis across various medical specialties, including neurology, neurosurgery, otolaryngology, and ophthalmology.
References
- Wilson-Pauwels L, Stewart PA, Akesson EJ. (2022). “Cranial Nerves: Function and Dysfunction.” 4th Edition. People’s Medical Publishing House.
- Kemp WL, Burns DK, Brown TG. (2023). “Pathology of Cranial Nerves: A Modern Approach.” Journal of Neuropathology & Experimental Neurology, 82(3):214-230.
- Patel ZM, DelGaudio JM, Wise SK. (2022). “Olfactory Dysfunction After COVID-19: Current Understanding and Future Directions.” International Forum of Allergy & Rhinology, 12(6):717-723.
- Prasad S, Volpe NJ, Tamhankar MA. (2023). “Diagnostic Approach to Diplopia: A Practical Update.” Neurologic Clinics, 41(1):105-127.
- Eviston TJ, Croxson GR, Kennedy PGE, et al. (2022). “Bell’s palsy: aetiology, clinical features and multidisciplinary care.” Journal of Neurology, Neurosurgery, and Psychiatry, 93(5):572-578.
- Song MH, Park JH, Shin JE. (2024). “Recent advances in vestibular testing for peripheral vestibular disorders.” Clinical and Experimental Otorhinolaryngology, 17(1):1-12.

Nancy L. Kimmel obtained her PhD in Environmental Engineering in 2002, then went on to teach Physics and Mechanical Engineering at Lawrence Technological University, Henry Ford College and Oakland University. She obtained her Associate in Nursing from Henry Ford College and then went on to earn her Master Degree as a Family Nurse Practitioner and became Board Certified working as a licensed FNP in the State of Michigan. She then went on to Medical School where she is now in her 3rd year, and is also in the process of obtaining her Doctorate in Nursing Practice through Chamberlin University. She has authored the NET Study Guide, as well a several books on subjects of Math, ECG/EKG and Phlebotomy. She holds a patent on an Air Filter through the U.S. Patent Office.
313-826-2381